1. Nkomo VT, Gardin JM, Skelton TN, et al. Lancet. 2006; 368: 1005–11.
2. Worldometer. Europe population (live). 2021. Available at: https://www.worldometers.info/world-population/europe-population/ [Accessed 24 March 2022].
3. Thourani V, Brennan J, Edelman J, et al. Struct Heart. 2021; 5(6): 608–18. DOI: 10.1080/24748706.2021.1988779.
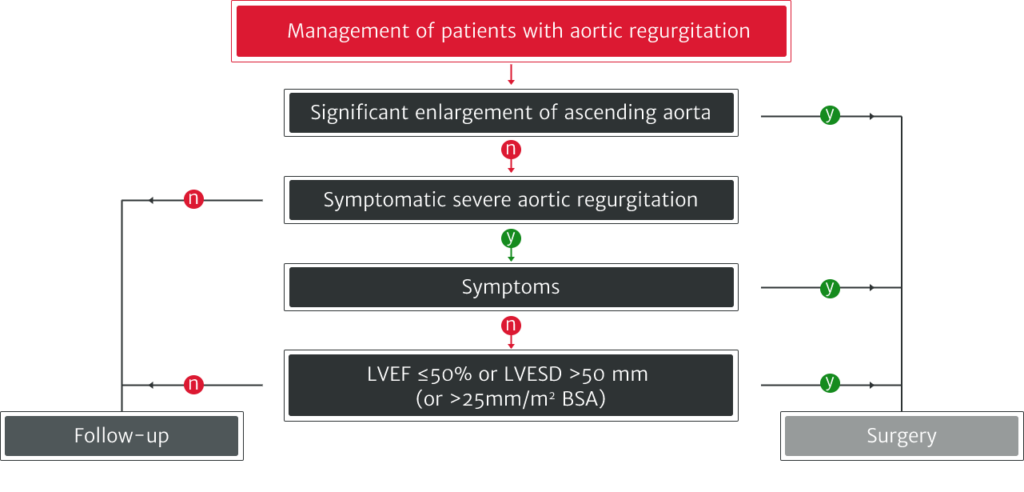
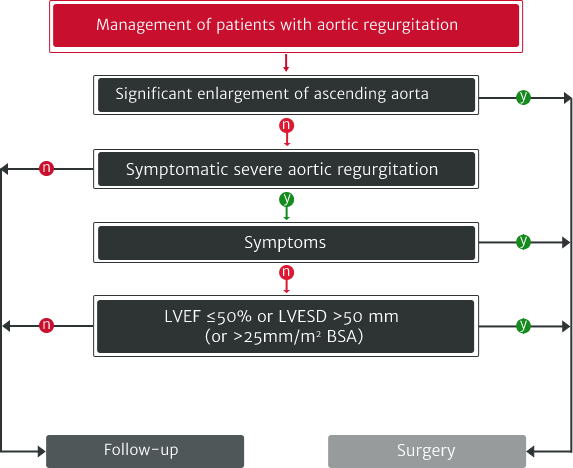
4. Vahanian A, Beyersdorf F, Praz F, et al. Eur Heart J. 2022; 43(7): 561–632.
5. d’Arcy JL, Coffey S, Loudon MA, et al. Eur Heart J. 2016; 37: 3515–22.
6. Yang LT, Michelena HI, Scott CG, et al. J Am Coll Cardiol. 2019; 73: 1741–52.
7. de Meester C, Gerber BL, Vancraeynest D, et al. JACC Cardiovasc Imaging. 2019; 12: 2126–38.
8. Iung B, Delgado V, Rosenhek R, et al. Circulation. 2019; 140: 1156–69.
9. Zoghbi WA, Adams D, Bonow RO, et al. J Am Soc Echocardiogr. 2017; 30: 303–71. doi:10.1016/j.echo.2017.01.007.
10. Akinseye OA, Pathak A, Ibebuogu UN. Curr Probl Cardiol. 2018; 43: 315–34.
11. Carabello BA. JACC. 2004; 44: 376–83.
12. Mentias A, Feng K, Alashi A, et al. J Am Coll Cardiol. 2016; 68: 2144–53.
13. Otto CM, Nishimura RA, Bonow RO, et al. J Am Coll Cardiol. 2021; 143: e35–71.
14. Alashi A, Mentias A, Abdallah A, et al. JACC Cardiovasc Imaging. 2018; 11: 673–82.
AR, aortic regurgitation; AS, aortic stenosis; SAVR, surgical aortic valve replacement; BSA, body surface area; CI, confidence interval; CMR, cardiac magnetic resonance; EACTS, European Association for Cardio-Thoracic Surgery; ESC, European Society of Cardiology; LV, left ventricle/left ventricular; LVEF, left ventricular ejection fraction; LVESD, left ventricular end-systolic diameter.