

How many people in Europe are estimated
to be living with AR?1,2
Delayed referrals for surgery can impact outcomes and reduce survival in people with aortic regurgitation (AR). 3 Guidelines emphasise that patients should undergo timely referral for comprehensive evaluation before irreversible damage occurs .4 Timely referral allows patients to receive successful surgical interventions.3

of the general population
are affected by AR 1

of the general population
are affected by aortic
stenosis (AS)1

people in Europe could be
living with AR1,2
In patients aged under 65 years, AR is more common than AS (AR 0.1%-0.7% versus AS 0.02%-0.2%).1
Around 50% of people aged >65 years have at least mild undetected valvular heart disease (VHD), and the number of people with clinically significant VHD, including AR, is expected to increase considerably over the next 50 years along with an ageing population.5
The 2021 ESC/EACTS VHD guidelines emphasise that patients should undergo timely referral for comprehensive evaluation before irreversible damage occurs.4
Patients must be referred to the heart team to be assessed for surgery without delay.4
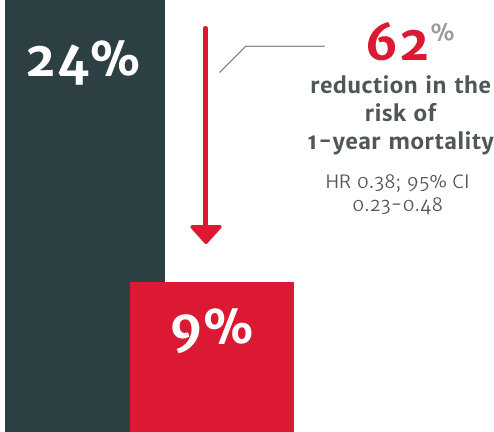
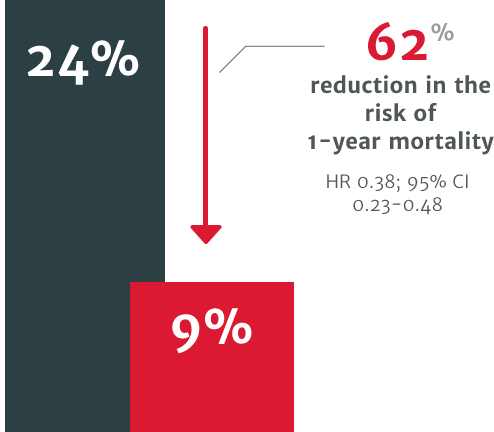
In a US retrospective study using the electronic health records of 4,608 symptomatic severe AR patients, patients who underwent surgical intervention for AR demonstrated improved survival versus patients who didn't receive intervention.3
62% relative risk reduction in the risk of 1-year mortality in patients who did not undergo SAVR within 1 year of diagnosis (24% mortality) compared to those who did (9% mortality).3


.png)
More than 40% of patients 65-69 years of age with VHD are not diagnosed.5
Early diagnosis can be challenging as obvious symptoms, such as angina and shortness of breath, usually occur after the optimal time for intervention.6,7
In patients with acquired AR, referral is sometimes delayed due to inappropriate evaluation of a patient's severity and symptoms.8
To evaluate AR, no single measurement or Doppler parameter can be used; multiple parameters must be integrated.9 For example, to fit the criteria of severe AR according to the ESC/EACTS 2021 guidelines, evaluation includes qualitative, semiquantitative and quantitative parameters.4
Stress testing is being used less and less, particularly
in asymptomatic cases with severe native VHD.8

For patients with untreated severe AR, the outlook is poor. This includes increased mortality.3
AR patients can suffer functional cardiovascular health decline.10 If treated conservatively, moderate to severe AR causes a 5-year and 10-year mortality rate of 25% and 50%, respectively.10
In moderate to severe AR patients, death usually occurs within 4 years after the onset of angina and 2 years after the onset of heart failure.10
Delayed referral could mean that patients no longer fully benefit from surgery.11
In a US retrospective study using the electronic health records of 4,608 symptomatic severe AR patients. The risk of mortality was found to be 2.7 times higher in symptomatic patients with severe AR who did not undergo surgery vs. those who received SAVR within one year of diagnosis (p<0.0001).3
In the same study, a patient's primary cardiologist was a strong determinant of the likelihood of receiving SAVR, even after controlling for potential confounders. Cardiologists with higher SAVR rates were shown to deliver improved 1-year survival for their severe symptomatic AR patients. Addressing this variability in treatment could improve patient outcomes.3
The ESC/EACTS 2021 guidelines were driven by studies showing improved survival outcomes with earlier surgical intervention.6,7,12
In one study based on the 2017 ESC/EACTS VHD guidelines, 10-year survival was found to be better if AR was surgically treated before guideline defined triggers, at the asymptomatic stage (patients operated on with a Class I guideline indication, n=204; Class IIa and IIb, n=66; before guideline defined triggers, n=86).7 Another study based on a previous version of the ACC/AHA guidelines from 2014, demonstrated better postoperative outcomes in patients who underwent surgery with less severe symptoms, compared to those that waited for guideline defined triggers (patients operated on with a Class I guideline indication, n=284; Class II, n=50; before guideline defined triggers, n=27).6
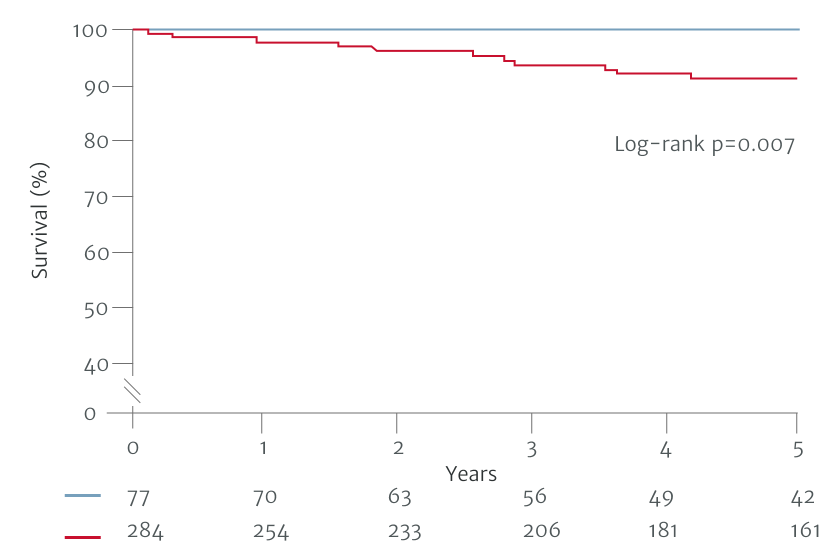

Patients with non-Class I indications for surgery had better postoperative survival.6
Adapted from Yang LT et al. 2019
Patients with non-Class I indications for surgery had better postoperative survival.6
62% relative risk reduction in the risk of 1-year mortality in patients who did not undergo SAVR within 1 year of diagnosis (24% mortality) compared to those who did (9% mortality).3
In a US retrospective study using the electronic health records of 4,608 symptomatic severe AR patients, patients who underwent surgical intervention for AR demonstrated improved survival versus patients who didn't receive intervention.3
62% relative risk reduction in the risk of 1-year mortality in patients who did not undergo SAVR within 1 year of diagnosis (24% mortality) compared to those who did (9% mortality).3
The ESC/EACTS 2021 guidelines recommend SAVR as the standard intervention in symptomatic severe AR (Class Ib), with several studies supporting this recommendation.4 Aortic valve repair may be considered in selected patients at experienced centres when durable results are expected (Class IIb).4 The same guidelines suggest TAVI may be considered in experienced centres for selected AR patients who are ineligible for SAVR.4
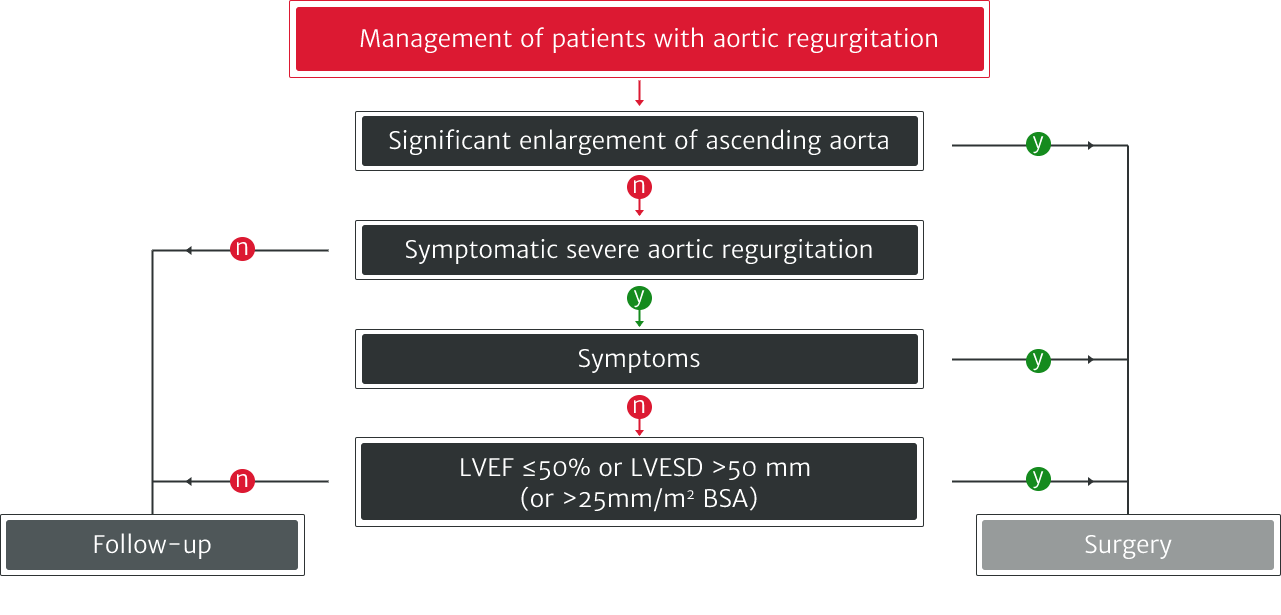
Adapted from Vahanian A et al. 2021.
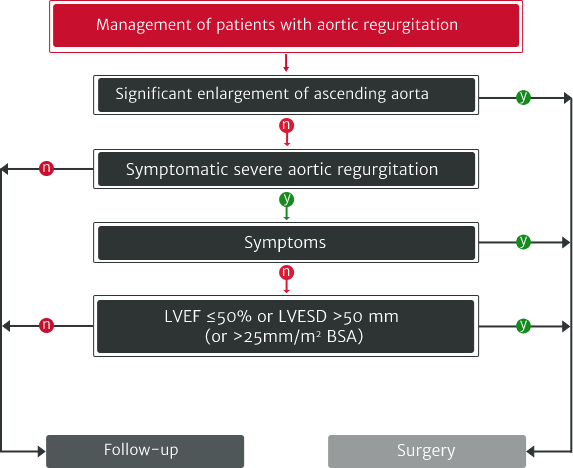
Adapted from Vahanian A et al. 2021.
There are several ways outcomes can be improved for patients with AR, from regular monitoring to earlier referral.4,8

Under-diagnosis in VHDs is a clear problem and may be linked to the underuse of stress testing, particularly in asymptomatic patients with severe native VHD.8 Multiple types of tests are needed, especially when physical examination and initial noninvasive testing are inconsistent.13

Further testing and regular monitoring can help to identify those who may require intervention by helping to establish the patient's disease severity.4,13 However, the VHD II 2017 survey reported that very few asymptomatic VHD patients undergo stress testing.8

Cardiac magnetic resonance (CMR) is becoming more popular for evaluating VHD, however less than 10% of patients are analysed in this way.8

New, more sensitive markers for LV dysfunction, such as LV global longitudinal strain, are being investigated. Several reports have also evaluated the potential role of newer indices like LV-global longitudinal strain, tissue Doppler and torsion.14
The ESC/EACTS 2021 guidelines were driven by studies showing improved survival outcomes with earlier surgical intervention.6,7,12


The ESC/EACTS 2021 guidelines were driven by studies showing improved survival outcomes with earlier surgical intervention.6,7,12
The Edwards Lifesciences AR podcasts are a series featuring some of the most eminent cardiac experts from across Europe, with a focus on the under-diagnosis and under-treatment of aortic regurgitation. They share their thoughts on best practice and suggestions on how to improve the standard of care.
To stay up to date, don't miss our podcast series on the definition, diagnosis and treatment of AR

AR, aortic regurgitation; AS, aortic stenosis; SAVR, surgical aortic valve replacement; BSA, body surface area; CI, confidence interval; CMR, cardiac magnetic resonance; EACTS, European Association for Cardio-Thoracic Surgery; ESC, European Society of Cardiology; LV, left ventricle/left ventricular; LVEF, left ventricular ejection fraction; LVESD, left ventricular end-systolic diameter.
